대한수면호흡학회
메뉴열기Good Sleep은 매년 1월, 5월, 9월 발간 예정입니다
AASM manual updates
AASM manual updates
The AASM Manual for the Scoring of Sleep and Associated Events
Summary of Updates in Version 2.6
January 10, 2020
부산성모병원 고태경
2020년 1월에 Sleep scoring 및 관련 events 에 대한 AASM Manual 이 업데이트 되어 Version 2.6 이 발행되었습니다. Version 2.6 에서는 Version 2.5 에 비해 총 14 부분의 additions and updates 가 있었습니다.
- Parameters to be reported for PSG 부분에서 synchronized PSG-video(Recommended), RWA(optional) 가 추가되었습니다.
- Technical and Digital Specifications 부분에서는 기존 내용을 명료하게 하기 위한 내용들이 추가되었습니다.
- Sleep Staging Rules 은 기본 내용의 변화는 없으며 기존 내용을 명료하게 하기 위해 설명 추가 및 Figures 가 추가되어 수정되었습니다.
- Cardiac rules 은 electrodes 위치를 명료하게 하기 위해 설명이 추가 되었습니다.
- Movement Rules 는 RBD 로 표기된 부분이 RWA(REM without atonia) 로 모두 수정되었으며 RWA scoring rules 일부 수정되었습니다.
- Respiratory rules 은 Adult and Children 모두 back-up rate 사용하는 PAP titration 시 respiratory event scoring 에 대한 내용이 추가 되었으며, Adult 에서는 intercostal EMG signal 에 대한 내용 및 figure 가 note 에 추가되었고, children 에서는 respiratory event 모니터링을 위해 dual thoracoabdominal PVDF belt 가 ACCEPTABLE 로 허용되었습니다.
아래 Table 1 에 14 곳의 변경 부분을 정리하였습니다.
| Version 2.5 | Version 2.6 | ||
| No. | Page | ||
| 1) | 8 | II. Parameters to be Reported for PSG (Section A) | Rule 10 추가 |
| 2) | 9 | II. Parameters to be Reported for PSG (Section E) | Rule 5 and Note 추가 |
| 3) | 13 | III. Technical and Digital Specifications (Section A) – Note 2 | Note 2 내용 update |
| 4) | 14 | III. Technical and Digital Specifications (Section B) – Rule 3 | Rule 3 내용 update |
| 5) | 23 | IV. Sleep Staging Rules, Part 1: Rules for Adults (Section F) – Rule 6 | Rule 6 내용 update |
| 6) | 31/29 | IV. Sleep Staging Rules, Part 1: Rules for Adults (Section I) – Rule 6c and Figure 15 | Rule 6c 내용 및 Figure 15 update |
| 7) | 37 | IV. Sleep Staging Rules, Part 3: Rules for Infants (Section B) – Rule 4 | Rule 4 내용 update (Figure 도 추가) |
| 8) | 47 | VI. Cardiac Rules (Section A) – Note 3 | Note 3 내용 update |
| 9) | 55 | VII. Movement Rules (Section G) | Section G 전체 내용 update |
| 10) | 57 | VIII. Respiratory Rules, Part 1: Rules for Adults (Section A) | Note and figure 추가 |
| 11) | 61 | VIII. Respiratory Rules, Part 1: Rules for Adults | Section H 추가 |
| 12) | 62 | VIII. Respiratory Rules, Part 2: Rules for children (Section B) | Rule 2e, 4e 추가 |
| 13) | 62 | VIII. Respiratory Rules, Part 2: Rules for children (Section B) | Rule 6c 추가 |
| 14) | 65 | VIII. Respiratory Rules, Part 2: Rules for children | Section I 추가 |
Table 1의 No. 에 따라 추가 또는 변경된 내용을 자세히 기술하였습니다.
1) Rule 10 이 추가
| 10. Synchronized PSG video | RECOMMENDED |
2) Rule 5 and Note 추가
| 5. REM without atonia (RWA) N1 | OPTIONAL |
| Note 1. If electing to measure RWA, the leads used to determine the presence of RWA should be included in the PSG report (e.g., chin, chin and lower limbs, chin and upper limbs). | |
3) Note 2. This applies to measured EEG and EOG electrode impedance. Electrode impedances should be rechecked during a recording when any pattern that might be artifactual appears. The AASM Scoring Manual currently does not specify maximum impedances for ECG or for EMG of the legs. However, it is suggested that the impedance be adjusted so that the baseline amplitude is minimized.
(파란색이 기존 Note 2. 내용에 더해서 추가된 부분입니다.)
4.
| 3. The capability of selecting sampling rates for each channel (Version 2.5) -> 3. The capability of providing the minimal recommended sampling rate (or higher) for all signals as specified in III.A.3 |
RECOMMENDED |
(파란색이 새로 변경된 부분입니다.)
5) 6. When an arousal interrupts stage R sleep and is followed by a low-amplitude, mixed-frequency EEG without posterior dominant rhythm AND with slow eye movements, score the portion of the record containing the eye movements as stage N1 even if the chin EMG activity remains low (at the stage R level). Continue to score stage N1 until there is evidence for another sleep stage (see G.2 for scoring stage N2 and I.3 for scoring stage R).
(파란색이 새로 변경된 부분입니다.)
6) 6c. An arousal occurs followed by low-amplitude, mixed-frequency EEG and slow eye movements (Score the epoch as state N1; if there are no Slow eye movements and chin EMG tone remains low, continue to score as stage R) (see Figure 15) (Version 2.5)
->
6c. When an arousal interrupts Stage R and is followed by a low-amplitude mixed-frequency EEG without posterior dominant rhythm AND slow eye movements, score the portion of the record containing the slow eye movements as Stage N1 even if the chin EMG activity remains low (at stage R level). Continue to score stage N1 until there is evidence for another stage, usually stage N2 (see G.2) or Stage R (see I.2 and I.3). If there are no slow eye movements and chin EMG tone remains low, continue to score as stage R (see Figure 15).
(파란색이 새로 변경된 부분입니다.)
- Version 2.5 Figure 15 와 비교해서 Figures 및 legends 는 A->B (변경부분만 파란색) 로 B->A 로 바뀌고, C, D (파란색으로 표시) 가 추가 되었습니다.
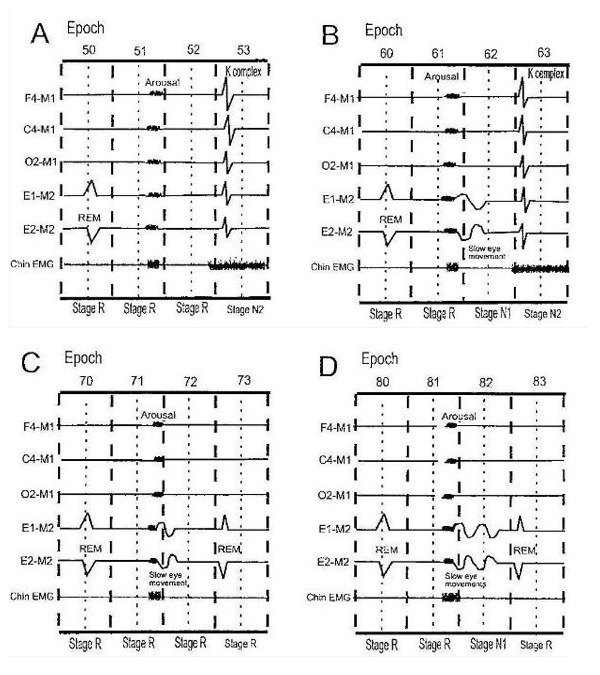
Figure 15. End of Stage R when an arousal is followed by slow eye movements. The EEG is assumed to contain low-amplitude, mixed-frequency activity unless otherwise depicted.
- Stage R is interrupted by an arousal followed by low-amplitude, mixed-frequency EEG without slow eye movements. Epoch 52 continues to be scored as stage R as the EEG shows a low-amplitude, mixed-frequency pattern, and the majority of the epoch contains low chin EMG tone (at the stage R level). Compare the effects of an arousal interrupting stage R with one interrupting N2 (Figure 8).
- Stage R is interrupted by an arousal followed by slow eye movements and low amplitude, mixed-frequency. Because slow eye movements are present following the arousal, Epoch 62 is scored as stage N1 even though chin activity is at the stage R level. Stage N1 continues until there is evidence for another sleep stage (here stage N2 in epoch 63).
- Stage R is interrupted by an arousal followed by slow eye movements and low amplitude, mixed-frequency EEG. However, the majority of epoch 72 does not contain slow eye movements and is scored as stage R based on rule I.3 as epoch 73 is definite stage R.
- Stage R is interrupted by an arousal followed by slow eye movements and low amplitude, mixed-frequency EEG with chin activity at the stage R level. Epoch 82 is scored as stage N1 even if the chin activity is at the stage R level as the majority of the epoch contains slow eye movements. Stage N1 continues until there is evidence of another sleep stage (here definite stage R in epoch 83).
(파란색이 새로 추가된 부분입니다.)
7) 4. Since behavioral patterns are extremely useful, synchronized video and audio recording is highly desirable. RECOMMENDED
(파란색이 새로 변경된 부분입니다. Optional->Recommended)
8) Note 3. While classically Lead II is derived from electrodes placed on the right arm and left leg, the negative electrode may be placed below the right clavicle at the mid-clavicular line and the positive electrode on the left lower chest at the anterior axillary line in the 6th or 7th intercostal space.
(파란색이 새로 추가된 부분입니다.)
9) 55 page 내용은 전체적으로 다음과 같이 바뀌었습니다. (RBD->RWA)
G. Scoring REM Without Atonia (RWA)
Scoring RWA is optional as noted in Parameters to be Reported (II.E).
- If electing to score RWA, score in accordance with the following definitions N1: RECOMMENDED
Excessive sustained muscle activity (tonic activity) in REM
: An epoch of stage R with at least 50% of the duration of the epoch having a chin EMG amplitude at least two times greater than the stage R atonia level (or lowest amplitude in NREM, if no stage R atonia present). Multiple segments may contribute to the total duration, but each segment must be greater than 5 seconds.
- If electing to score RWA, score and epoch as exhibiting RWA when one of the following is present:N1,N2,N3,N4,N5
- Excessive sustained muscle activity in REM in the chin EMG (as defined in rule VII.G.1) RECOMMENDED
- Excessive transient muscle activity during REM in the chin or limb EMG (as defined in rule VII.G.1) RECOMMENDED
- At least 50% of 3 second mini-epochs contain any chin activity (as defined in rule VII.G.1) or limb EMG activity (bursts of EMG activity 0.1-5.0 seconds in duration and at least two times as high in amplitude as the stage R atonia level or lowest amplitude in NREM, if no stage R atonia is present).N2,N3 ACCEPTABLE
- If electing to score RWA, score the RWA index as the % of stage R epochs that meet criteria in rule VII.G.2.N3 OPTIONAL
Excessive transient muscle activity (phasic activity) in REM N2: In a 30-second epoch of stage R divided into 10 sequential 3-second mini-epochs, at least 5 (50%) of the mini-epochs contain bursts of transient muscle activity in the chin or limb EMG. In RWA, excessive transient muscle activity burst are 0.1-5.0 seconds in duration and at least two times as high amplitude as the stage R atonia level ( or lowest amplitude in NREM, if no stage R atonia is present).
Any chin EMG activity N3: Activity with a minimum amplitude two times greater than the stage R atonia level (or lowest amplitude in NREM, if no stage R atonia is present) without regard to the duration of the activity (including bursts of 5 to 15 seconds).
|
Note 1. The definitions of sustained and transient muscle activity are based on duration rather than morphology. Although transient activity is often composed of intermittent brief bursts, activity with relatively constant amplitude that otherwise meets criteria VII.G.2 qualifies as transient activity. Note 2. If a periodic limb movement (PLM) is scored as part of a PLM series, it should not be counted in determining if an epoch has RWA. Note 3. Based on SINBAR (Sleep Innsbruck Barcelona) Group recommended criteria.1 Note 4. Epochs containing RWA with sustained chin activity as defined above may not meet criteria for stage R but in these cases, the epoch can still be scored as stage R if other criteria for stage R are met or if the epoch is contiguous with an epoch scored as stage R. Note 5. If electing to measure RWA, the leads used to determine the presence of RWA should be included in the PSG report (e.g., chin, chin and lower limbs, chin and upper limbs). |
Reference
- 1. Frauscher B; Iranzo A; Gaig C; Gschliesser V; Guaita M; Raffelseder V; Ehrmann L; Sola N; Salamero M; Tolosa E; Poewe W; Santamaria J; Högl B; SINBAR (sleep Innsbruck Barcelona) Group. Normative EMG values during REM sleep for the diagnosis of REM sleep behavior disorder. SLEEP 2012;35(6):835-847.
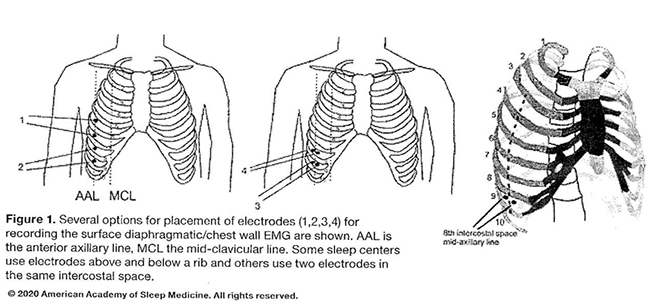
10) Note 4 가 추가(Figure 1. 포함) 되었으며, version 2.5의 Note 4->5, Note 5->6, Note 6->7 로 변경되었습니다.
Note 4. A surface diaphragmatic/intercostal EMG signal may be used for detection of respiratory effort during apnea, hypopnea, or RERA events to complement effort belt signals when unambiguous inspiratory EMG bursts are visible during normal breathing. Various electrode placements have been used in the published literature. Some of the placements are illustrated in Figure 1. If one electrode placement does not yield a good signal, others may be tried. Some placements utilize an electrode above and another below a rib while others place both electrodes in the same intercostal space. Positions at the mid-clavicular, anterior axillary, and mid-axillary lines have been used. The 6th, 7th, or 8th intercostal space is commonly used but slightly higher or lower may result in a better signal in some patients. While low and high filter settings recommended for recording of the anterior tibial EMG can be used (low 10 Hz, high 100 Hz), ECG artifact will be reduced if a low filter setting of 25 to 40 Hz is used. Some polysomnography programs have an option for removal of ECG artifact from EMG signals.
11) H. Special Circumstances for Scoring Respiratory Events
Scoring respiratory events during a positive airway pressure (PAP) titration using a backup rate:
1. Score a respiratory event occurring during PAP device-triggered breaths as a central apnea if all of the following criteria are met:N1 RECOMMENDED
- There is a decrease in the PAP flow signal meeting apnea criteria
- Device triggered pressure pulses (pressure support) occur during the event
- There is no evidence of spontaneous (patient triggered) respiratory effort during the event
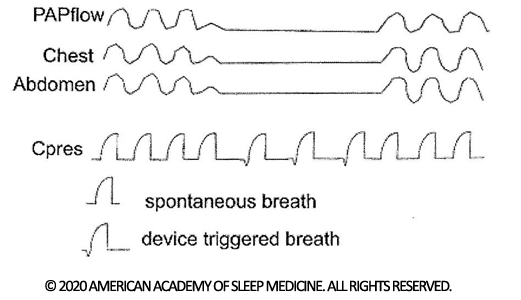
Figure 7. A central apnea during PAP device-triggered breaths. A reduction in PAP flow meeting criteria for an apnea is present. Cpres is the delivered pressure signal from the PAP device. The small downward artifact identifies a device-triggered pressure pulse. During apnea, several device-triggered pressure pulses are note in the absence of deflections in the chest or abdominal effort belt signals.
| Note 1. Laboratories should check with the manufacturer of their polysomnogram recording equipment to determine whether it is capable of displaying device-triggered pressure pulses and/or the proper configuration required to display them. |
12) 2e. PVDFsum ACCEPTABLE
4e. PVDFsum ACCEPTABLE
13) 6c. dual thoracoabdominal PVDF belts ACCEPTABLE
14) 11) H 추가된 내용과 동일
I. Special Circumstances for Scoring Respiratory Events
Scoring respiratory events during a positive airway pressure (PAP) titration using a backup rate:
1. Score a respiratory event occurring during PAP device-triggered breaths as a central apnea if all of the following criteria are met:N1 RECOMMENDED
- There is a decrease in the PAP flow signal meeting apnea criteria
- Device triggered pressure pulses (pressure support) occur during the event
- There is no evidence of spontaneous (patient triggered) respiratory effort during the event
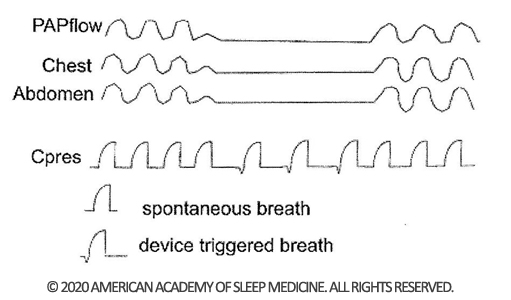
Figure 1. A central apnea during PAP device-triggered breaths. A reduction in PAP flow meeting criteria for an apnea is present. Cpres is the delivered pressure signal from the PAP device. The small downward artifact identifies a device-triggered pressure pulse. During apnea, several device-triggered pressure pulses are note in the absence of deflections in the chest or abdominal effort belt signals.
| Note 1. Laboratories should check with the manufacturer of their polysomnogram recording equipment to determine whether it is capable of displaying device-triggered pressure pulses and/or the proper configuration required to display them. |
Reference
- Berry RB, Brooks R, Gamaldo CE, et al. for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Darien, IL: American Academy of Sleep Medicine; 2018. Version 2.5.
- Berry RB, Brooks R, Gamaldo CE, et al. for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Darien, IL: American Academy of Sleep Medicine; 2020. Version 2.6.
- The AASM Manual for the Scoring of Sleep and Associated Events Summary of Updates in Version 2.6.